The Governance Failure Behind the Global Health Funding Crisis



The world’s growing instability in health financing is sometimes described as a budget problem. In reality, it is a far more complex issue: a governance crisis within the institutions responsible for global public health. While the consequences are increasingly visible in primary healthcare systems around the world, the underlying challenge concerns how global health institutions are financed, governed, and held accountable.
Governance, here, is defined as decision-making authority, financial control, institutional accountability, and priority-setting power within transnational public health institutions. The unfolding health financing crisis has revealed structural tensions that have persisted for years yet remained politically manageable during periods of relative funding stability.
That has changed. The consequences are no longer confined to balance sheets and budget negotiations; they are increasingly visible in clinics, laboratories, vaccination campaigns, and emergency response systems around the world.
World Health Organization (WHO) officials now warn that the agency faces one of the largest financing gaps in its modern history. According to Health Policy Watch, WHO's projected budget shortfall for the 2026–2027 cycle approaches $1.9 billion. Reuters separately reported WHO Director-General Tedros Adhanom Ghebreyesus's warning that global health financing is experiencing the "greatest disruption in memory," forcing hiring freezes, operational reductions, and programmatic restructuring across multiple regions.
At the same time, broader reductions in official development assistance are constraining vaccination campaigns, maternal health initiatives, and disease surveillance systems in low-income countries already operating with limited clinical capacity. The World Health Organization has warned that external health aid is projected to decline by 30 to 40 percent compared with 2023 levels, with some countries reporting significant disruptions to maternal care, immunization programs, emergency preparedness, and disease surveillance systems. The Kaiser Family Foundation notes that the United States historically contributed a substantial share of WHO financing, making recent withdrawal and funding suspension measures particularly consequential for long-term institutional planning.
The challenge extends beyond WHO. Over the past year, UN agencies and major global health partnerships have also faced severe funding shortfalls as wealthy donor governments reduce foreign aid commitments and redirect spending toward domestic political priorities, defense expansion, migration management, and debt pressures. The consequences are already visible in strained Ebola response operations in Central Africa, disruptions to vaccine delivery programs, shortages of frontline healthcare workers, and weakening disease surveillance capacity across multiple regions. Yet the present turmoil did not emerge suddenly. It reflects longstanding weaknesses in how global health institutions are financed and governed.
From this perspective, the current instability may represent less a crisis of institutional survival than a moment of institutional reassessment. Whether the emerging transition produces more effective forms of cooperation and renewed institutional legitimacy, greater fragmentation and competitive regionalism, or the displacement of existing organizations by alternative governance arrangements remains uncertain.
The future of global health governance will not be determined solely by the availability of funding, but by whether international institutions can align authority, responsibility, and resources in ways that sustain both effectiveness and legitimacy. The present crisis has exposed vulnerabilities that were long recognized but insufficiently addressed. Whether governments, donors, and international organizations possess the political will to undertake the reforms necessary to address those weaknesses remains an open question. What is clear is that financing can no longer be treated as a technical or administrative concern. It has become a defining test of institutional stewardship, operational independence, and the capacity of global health institutions to fulfill the responsibilities entrusted to them.
At the center of the problem is an institutional contradiction: governments increasingly describe pandemics and infectious disease threats as matters of national security while financing the institutions responsible for pandemic prevention through unstable voluntary appropriations vulnerable to domestic political cycles.
The leadership language surrounding this crisis is itself revealing. WHO officials have urged countries to “transition away from aid dependency” and strengthen domestic financing. That recommendation is not wrong. Stronger domestic financing and greater national self-sufficiency should remain important long-term objectives for many health systems.
Yet as a governance response, the recommendation is incomplete. Many countries developed essential public health services within financing structures that donor governments, multilateral organizations, and global health institutions actively supported for decades. Leadership requires not only recognizing dependency, but responsibly managing the transition away from it. Abrupt funding reductions shift the burden of adjustment onto health systems least able to absorb the shock while leaving insufficiently examined the institutional architecture that created the dependency in the first place. The governance question is not simply whether countries should become more self-reliant. It is whether those who helped build the existing system exercised adequate stewardship in planning for its transition.
Historically, WHO was designed as a multilateral public institution funded primarily through mandatory member-state contributions. Over time, however, that model eroded. Today, much of WHO’s budget comes from voluntary earmarked donations provided by governments, philanthropies, and international partnerships.
Because voluntary contributions are frequently earmarked for specific initiatives, donor states and private actors increasingly influence how resources are allocated. Critics argue this arrangement weakens WHO’s independent priority-setting authority and limits institutional flexibility during emergencies. Over time, member states and donor institutions collectively accepted this arrangement despite longstanding concerns regarding dependency, financial volatility, and institutional autonomy.
The consequences of this financing model extend beyond budgets and balance sheets. They reveal a persistent misalignment between institutional responsibilities and the resources available to fulfill them. Reflecting on leadership in complex health systems, Dr. Abdihamid I. Ahmed, a physician and UNICEF specialist in primary healthcare and health systems strengthening, observed that "leadership is less about control and more about interpretation and alignment." That observation is particularly relevant to the current crisis. For decades, global health institutions were expected to coordinate surveillance, preparedness, vaccination, and emergency response, yet the financing structures supporting those responsibilities remained vulnerable to shifting donor priorities and political cycles. The resulting challenge is not simply financial dependency, but a longstanding failure to align authority, responsibility, and resources.
The issue is not merely that donors have withdrawn funds. The more consequential governance question is why governments, donor institutions, and global health organizations continued to rely upon a financing model whose vulnerabilities had long been recognized. Over time, dependency ceased to be a temporary feature of the system and became embedded within its architecture. Effective governance requires that responsibility, authority, and resources remain aligned. In global health, they often do not.

The persistence of this model reflects a broader governance failure. The risks associated with donor dependency, earmarked financing, and institutional vulnerability were neither hidden nor unforeseen. Yet no single actor possessed both the authority and the incentive to fundamentally reform the system. Member states retained influence through discretionary funding, institutions adapted to chronic financial uncertainty, and donors preserved the ability to direct resources toward preferred priorities. The result was a financing architecture that remained operational but increasingly vulnerable.
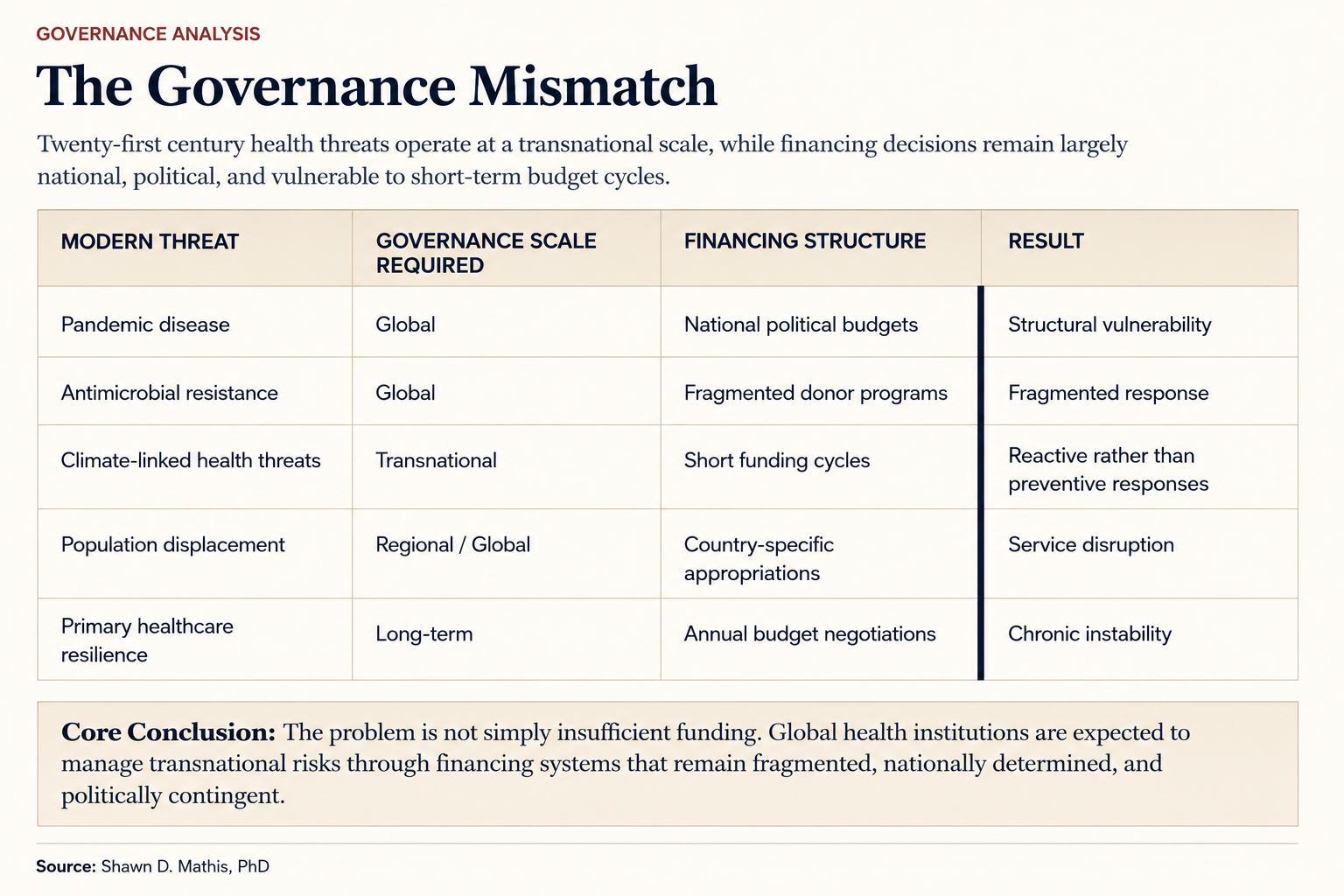
This structure creates a clear governance dilemma. WHO is expected to coordinate cross-border disease surveillance, emergency response operations, and public health guidance for nearly every nation on earth. Yet its ability to independently allocate resources often depends on the political preferences of a relatively small number of donor governments and institutions. Responsibility has become global, while many financing decisions remain national and political.
The significance of that mismatch extends beyond WHO itself. Pandemics, antimicrobial resistance, climate-linked disease outbreaks, and mass displacement are transnational challenges requiring sustained international coordination. Yet the institutions responsible for managing those risks continue to operate within financing arrangements vulnerable to shifting political priorities and fiscal cycles. The architecture of dependency was not created by a single institution or government. It emerged gradually through a system that normalized financial vulnerability while expanding institutional responsibility.
The consequences of governance failure are rarely abstract. When major governments reduce aid budgets or shift priorities, international health institutions experience immediate operational constraints. The resulting disruptions reveal more than a funding shortfall; they expose the consequences of governance arrangements that allowed essential public health functions to remain dependent upon politically contingent financing.
Those consequences are increasingly measurable. WHO has warned that funding reductions are already resulting in staff layoffs, clinic closures, interruptions in childhood immunization campaigns, reduced access to tuberculosis and HIV treatment, and diminished emergency outbreak response capacity across multiple regions. In some humanitarian settings, aid agencies report reductions in frontline healthcare staffing reaching double-digit percentages within a single fiscal year.
The numbers make the consequences of governance failure difficult to ignore. WHO has reported that external health aid is projected to fall by 30 to 40 percent compared with 2023 levels, with maternal care, vaccination, disease surveillance, and emergency preparedness reduced by as much as 70 percent in some countries. UNAIDS has warned that U.S. funding cuts alone could contribute to 6.6 million additional HIV infections and 4.2 million AIDS-related deaths by 2029 if the gap is not replaced. Médecins Sans Frontières has likewise reported closed clinics, disrupted vaccination programs, and interrupted care in crisis settings following U.S. aid cuts.
Several international health organizations, including WHO, UNAIDS, and Médecins Sans Frontières, have warned that reductions in donor funding threaten to reverse decades of progress in disease control, vaccination coverage, maternal health, and outbreak preparedness. Their concerns extend beyond the scale of the cuts themselves to the governance model that permits essential public health functions to depend upon discretionary political appropriations.
The OECD has projected significant declines in official development assistance following earlier reductions in 2024, warning that global aid flows may continue shrinking amid rising geopolitical tensions and fiscal pressures. The prospect of sustained funding contraction raises questions not only about resource availability, but about the resilience of governance arrangements that remain dependent upon increasingly uncertain political commitments.
The practical implications are already visible. Recent reporting on the Ebola outbreak in the Democratic Republic of the Congo has linked delays in detection and response to a weakened epidemiological surveillance chain following significant reductions in international health funding. The challenge is not merely the scale of the outbreak itself, but the difficulty of sustaining coordinated international response capacity when the institutions responsible for surveillance and preparedness face growing financial uncertainty.
This instability has exposed a deeper mismatch between modern health threats and twentieth-century institutional design. Pandemics, climate-linked disease outbreaks, antimicrobial resistance, and mass displacement are transnational problems requiring sustained international coordination. Yet the institutions tasked with managing those risks remain financially dependent on fragmented annual budget negotiations within individual nation-states. When financing structures fail to evolve alongside expanding institutional responsibilities, governance failures become operational failures.
The operational consequences extend beyond administrative disruption. Delayed outbreak detection, weakened laboratory systems, and reduced staffing increase transmission risks and make outbreaks more difficult and expensive to contain.
These crises expose the practical effects of governance dependency. When funding is unstable or politically constrained, organizations are often forced to prioritize immediate crisis response over long-term system resilience. Foundational investments such as laboratory infrastructure, workforce development, sanitation systems, and local clinical capacity are frequently underfunded because they lack the political visibility and urgency of high-profile emergency interventions.
In several aid-dependent health systems, donor reductions have forced the closure of community clinics, the suspension of vaccination campaigns, and layoffs affecting thousands of healthcare workers and support staff. Programs addressing HIV, tuberculosis, maternal health, and other essential services have reported disruptions affecting millions of beneficiaries. In many low-income regions, diminished external funding has weakened community health worker networks, restricted access to maternal care, and interrupted routine immunization schedules and sanitation programs. WHO has warned that disruptions in essential health services can contribute to increases in preventable mortality, particularly among children under five and medically vulnerable populations. Ultimately, the consequences of governance failure are borne not by institutions or donors, but by the communities whose health and well-being depend upon the continuity of essential public services.
The structure of earmarked financing further intensifies this problem. Governments and donors frequently direct resources toward specific diseases or initiatives that produce measurable political or public relations value. The result is a fragmented system in which institutional priorities may reflect donor preferences more than coordinated long-term public health planning.
Private philanthropy has also acquired unprecedented influence within international health governance. Large foundations now finance substantial portions of disease eradication initiatives, vaccine programs, and research infrastructure. While these organizations provide essential support, some public health scholars have questioned whether international priority-setting is increasingly shaped by donor priorities rather than collective member-state deliberation. The concern is not philanthropy itself, but the extent to which institutions charged with exercising independent public authority become dependent upon external actors for the resources required to fulfill their mandates.
An analysis from IQVIA argues that global health governance is entering a period of significant transition as authority, financing, and priority-setting become less exclusively Western-led. Emerging powers are expanding their influence through investment, production capacity, pandemic preparedness initiatives, and regional partnerships, contributing to a more diffuse distribution of financial and political influence across the global health system. The issue is not the emergence of new actors itself. A more diverse financing landscape may strengthen resilience and broaden participation in global health governance. The governance challenge is that shifts in financial influence often reshape priority-setting authority, raising questions about how institutional independence can be preserved when resources and decision-making power become increasingly dispersed across competing political actors.
Even within the broader United Nations system, financial instability is accelerating calls for structural reform. The significance of these developments extends beyond budget management. The Lusaka Agenda, which emerged from a multi-stakeholder process examining the future of global health initiatives, argues that long-term sustainability requires stronger country ownership, more durable financing arrangements, and mutual accountability across the global health ecosystem. The current crisis suggests that such reforms are no longer merely desirable; they have become necessary. When financial pressures begin to shape organizational design, staffing decisions, and institutional priorities, dependency ceases to be merely a financing challenge and becomes a governance challenge. Over time, institutions risk losing not only operational capacity, but also the independence necessary to define priorities, allocate resources, and exercise authority in accordance with their public mandates rather than the preferences of those controlling essential sources of funding.
The economic implications are equally significant. The World Bank estimates that major pandemics can impose trillions of dollars in global economic losses through workforce disruption, supply chain instability, healthcare system strain, and reduced trade activity. Yet the institutions responsible for early detection and coordinated response continue to operate under financing structures vulnerable to annual political retrenchment.
Identifying the governance failure is only part of the challenge. The more difficult question is how transnational public health institutions should be governed going forward. If the present crisis reveals a failure of stewardship, then meaningful reform cannot be limited to replacing lost funding. It must address the structural conditions that allowed known vulnerabilities to become embedded within the architecture of global health governance.
Authority must be aligned with resources. Institutions cannot be held responsible for outbreak preparedness, disease surveillance, vaccination coordination, and primary healthcare support while remaining dependent on unstable funding mechanisms outside their control. Core public health functions should be supported through financing arrangements that better reflect the responsibilities these institutions are expected to fulfill.
Stewardship itself must become more accountable. The risks associated with donor dependency, earmarked financing, and institutional vulnerability were widely recognized long before the present crisis emerged. Governing boards, member states, and institutional leadership should be expected to regularly assess, publicly report, and act upon structural risks that threaten long-term institutional viability.
Primary healthcare should be treated as strategic infrastructure rather than discretionary expenditure. Community clinics, vaccination systems, maternal health services, disease surveillance networks, and frontline health workers represent foundational public assets. When financing instability undermines those systems, the consequences extend far beyond public health. They affect social stability, economic resilience, institutional legitimacy, and public trust.
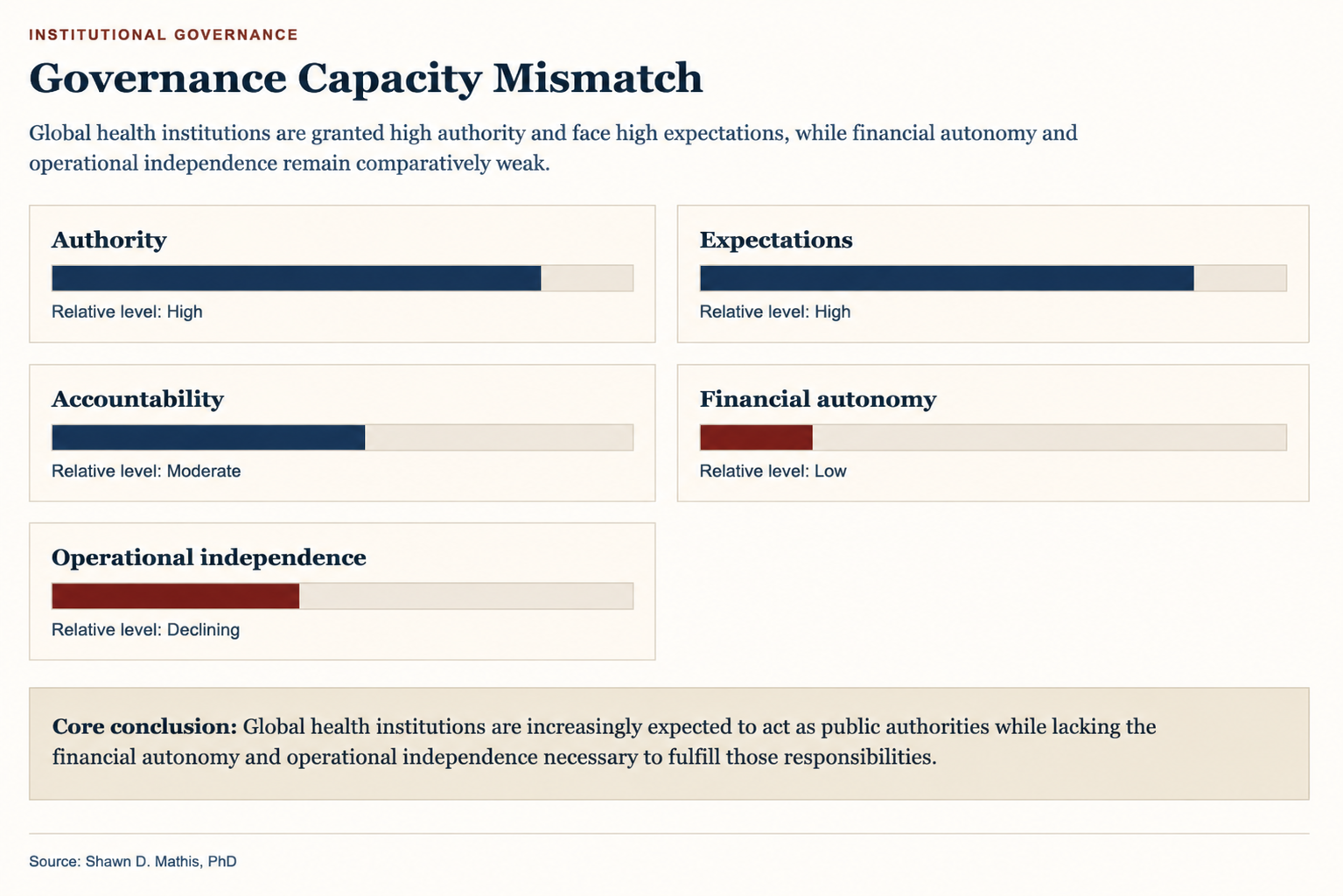
The present debate ultimately concerns whether international health institutions can exercise meaningful independent authority while remaining financially dependent upon discretionary political support from member states and private donors.
The contradiction is not simply financial. International health institutions are treated as global public authorities when they issue guidance, coordinate surveillance, and define health priorities, yet they remain financially dependent upon the shifting priorities of states, donors, and philanthropic actors. That dependence shapes not only what these institutions can do, but also what they are able to know, prioritize, and imagine about the future of global health governance.
That question will shape more than bureaucratic budgets. Future pandemic preparedness, outbreak response capacity, vaccine coordination, and disease surveillance systems will depend in part on whether international institutions possess sufficient financial stability and operational independence to act before crises escalate.
The current instability suggests that the post-1945 architecture of global health governance may be entering a significant institutional transition. Whether that transition produces stronger coordination and more durable financing structures—or greater fragmentation and political competition—remains uncertain.
What is already clear is that financing is no longer merely an administrative issue within global health governance. It has become a central measure of institutional authority, operational independence, and political legitimacy—and, ultimately, of whether global health institutions can fulfill the responsibilities they have been entrusted to carry.