When Expertise Loses Authority: The Crisis of American Public Health Legitimacy



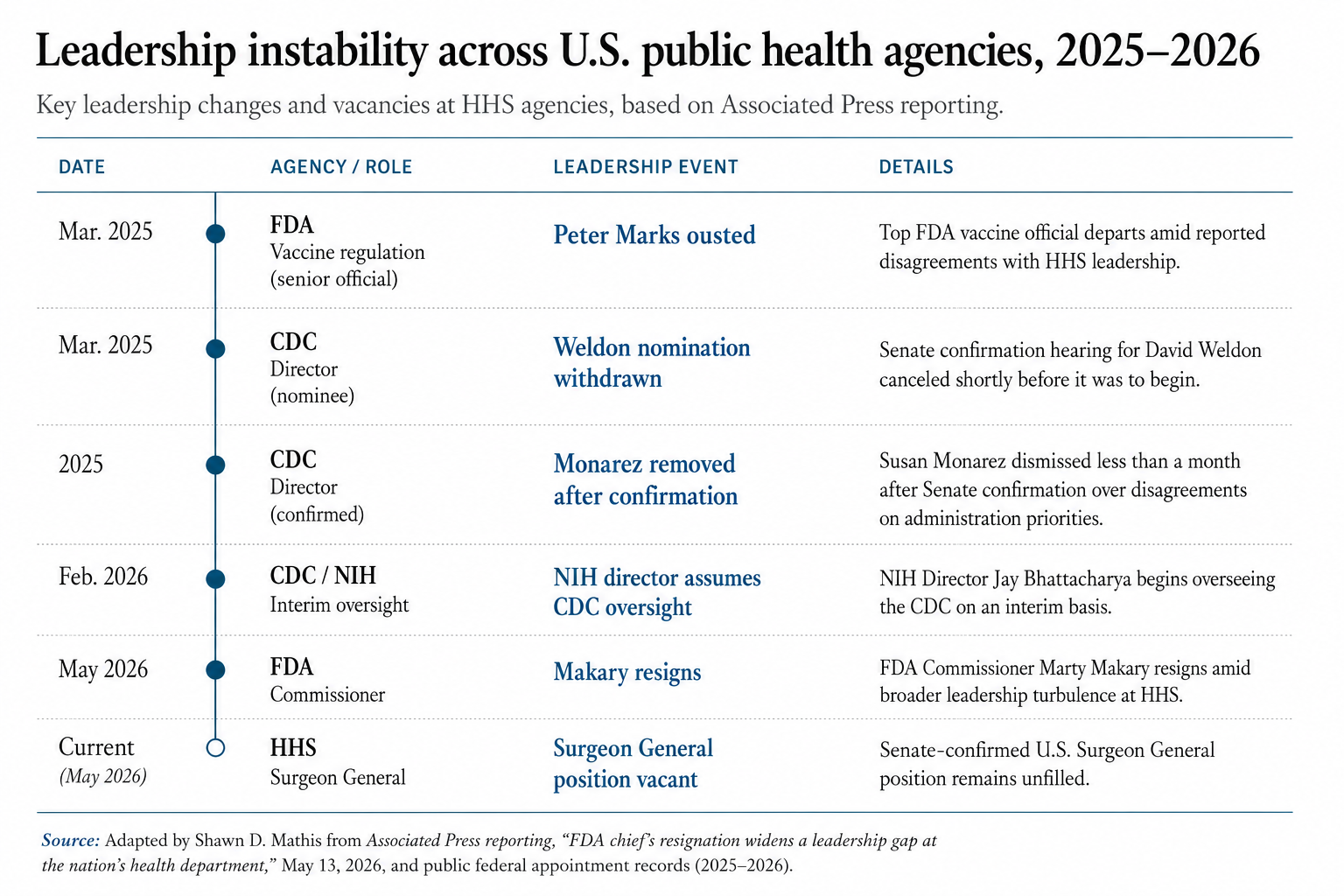
The resignation of Food and Drug Administration (FDA) Commissioner Martin Makary would ordinarily constitute little more than another episode in Washington’s familiar cycle of bureaucratic turnover. Senior officials depart. Interim appointees rotate through agencies. Administrations recalibrate priorities. Yet the significance of the present moment lies not in the resignation itself, but in the broader institutional condition it reveals. Across the Department of Health and Human Services (HHS), leadership vacancies, scientific resignations, interim appointments, and contested authority structures now converge simultaneously.
This is not merely administrative instability. It is evidence of a deeper crisis in the architecture of American public health governance: the gradual erosion of institutional legitimacy within the expert bodies upon which modern healthcare systems depend.
The Associated Press reporting makes the surface facts clear enough. The FDA lacks stable leadership. The Centers for Disease Control and Prevention (CDC) has cycled through temporary oversight arrangements. The Surgeon General position remains unfilled. Senior scientific officials have departed amid accusations of political interference and ideological conflict. On its face, this appears to be a story about personnel management and partisan disagreement. In reality, it reflects a more consequential development: the weakening of the postwar settlement between democratic politics and expert authority.
Modern healthcare systems cannot function without technocratic institutions. Agencies such as the FDA, CDC, and National Institutes of Health (NIH) exist because industrial societies long ago exceeded the capacity of ordinary democratic mechanisms to evaluate pharmaceutical safety, epidemiological risk, biomedical research, and national disease coordination directly. Expertise became institutionalized not as a luxury, but as a structural necessity.
Yet expert institutions possess a peculiar vulnerability. Unlike armies or police forces, they govern primarily through credibility rather than coercion. Their authority depends upon public confidence that decisions are procedurally disciplined, scientifically competent, and insulated from overt factional pressure. Pharmaceutical markets obey FDA rulings because they presume institutional continuity. Citizens comply with public health guidance because they trust the legitimacy of the issuing authority. Hospitals coordinate around CDC recommendations because the institution historically represented a relatively stable repository of scientific judgment.
Once those assumptions weaken, the operational capacity of the healthcare system itself begins to degrade.
This is the significance of the present turmoil at HHS. The problem is not simply that leadership positions remain vacant. The problem is that the institutional conditions necessary for trusted healthcare governance are becoming increasingly unstable.
The conventional interpretation of this crisis is unsatisfactory. One side argues that technocratic institutions became politically ideological, culturally insulated, and insufficiently accountable to democratic oversight. The opposing side insists that populist politics has corrupted scientific administration and weakened evidence-based governance. Both arguments contain elements of truth. Neither adequately explains the structural reality.
The central reality is that the crisis emerged not simply because institutions were attacked from the outside, but because many institutions gradually ceased behaving in the restrained and institutionally neutral manner that originally justified public deference toward them.
For decades, public health institutions benefited from the prestige accumulated during an unusually high-trust period in American life. Citizens broadly assumed that agencies such as the FDA and CDC operated primarily as technocratic bodies: politically restrained, scientifically disciplined, and culturally neutral. That legitimacy was real. But over time, many institutions retained the language and authority of neutrality even as they increasingly absorbed the assumptions, moral frameworks, and ideological instincts of the professional classes that staffed them.
The problem, therefore, is not that these institutions became fundamentally illegitimate. Nor is it true that expertise itself lost value. The central issue is that institutional behavior increasingly diverged from institutional self-description. Agencies that once presented themselves as narrow administrative bodies gradually expanded into broader forms of social and moral management while continuing to claim the older legitimacy associated with politically disinterested expertise.
The legitimacy crisis did not emerge solely because institutions made mistakes. It emerged because institutions increasingly appeared unwilling to recognize the limits of their own authority. Scientific expertise can inform democratic societies. It cannot permanently substitute for them. Once administrative agencies begin treating dissent not merely as error but as moral deviance, they cease to appear institutionally neutral and begin to appear politically sovereign.
The COVID-19 pandemic did not create the legitimacy crisis, but it accelerated and exposed it dramatically. Public health agencies often communicated legitimate uncertainty with excessive certainty. Dissent was at times treated not merely as disagreement, but as irresponsibility or illegitimacy. Scientific institutions accustomed to procedural authority increasingly entered the terrain of political persuasion, cultural signaling, and moral instruction. In doing so, they weakened the perception of neutrality upon which their authority ultimately depended.
When trust deteriorates, even technically sophisticated systems become operationally fragile.
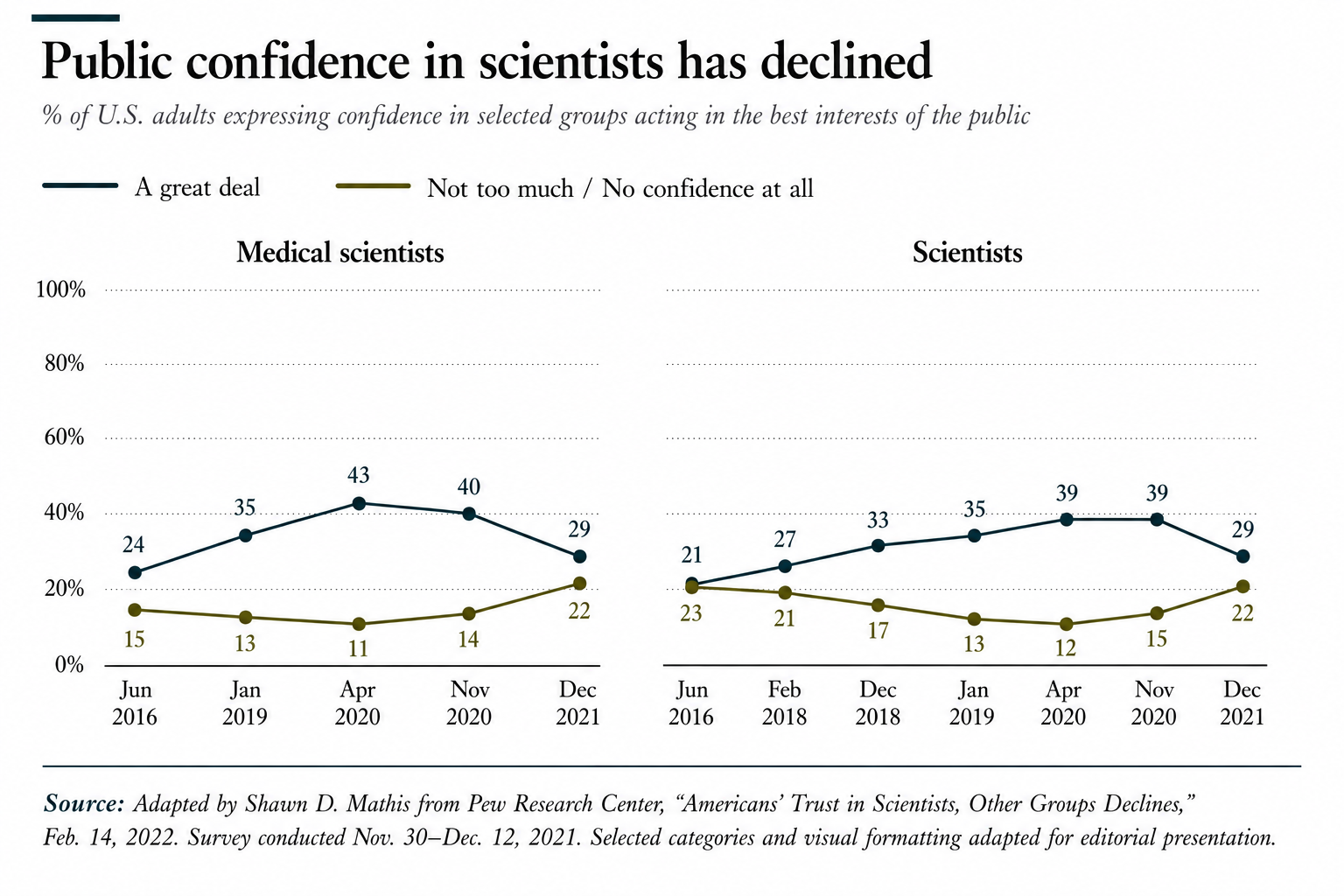
The deterioration is measurable, not merely rhetorical. Pew Research Center data shows that public confidence in medical scientists rose sharply during the initial phase of the COVID-19 crisis, only to decline afterward to levels below those recorded before the pandemic itself. As Pew reported, “Overall, 29% of U.S. adults say they have a great deal of confidence in medical scientists … down from 40% who said this in November 2020.” Even more strikingly, Pew concluded that “current ratings of medical scientists and scientists have now fallen below where they were in January 2019, before the emergence of the coronavirus.”
The paradox is difficult to ignore: public health institutions exercised the greatest degree of authority in modern American history during precisely the period in which public confidence in them began materially to deteriorate.
Yet the reaction against these institutions has frequently proven equally corrosive. Legitimate criticism of institutional overreach gradually merged with indiscriminate suspicion toward expertise itself. Public health agencies were no longer viewed as flawed institutions requiring reform, but increasingly as inherently compromised instruments of ideological power. Once institutions lose the presumption of procedural good faith entirely, competent governance becomes extraordinarily difficult.
The result is a legitimacy spiral. Institutions respond defensively to public distrust. Public distrust intensifies in response to institutional defensiveness. Political actors exploit the resulting instability for factional advantage. Scientific agencies then become progressively more politicized precisely because they are accused of politicization.
This dynamic now extends far beyond healthcare. Gallup’s long-running confidence surveys show that declining trust is not confined to public health agencies alone, but extends across Congress, higher education, media organizations, business leadership, and other core institutions of American civic life.
For much of the twentieth century, advanced Western societies operated under a relatively stable managerial consensus in which citizens broadly accepted that specialized institutions possessed legitimate authority within domains requiring technical competence. Courts interpreted law. Central banks managed monetary policy. Universities produced expert knowledge. Public health agencies mediated scientific complexity on behalf of society.
That arrangement depended upon several assumptions: that elites were broadly competent, that institutions operated within recognizable professional norms, and that bureaucratic authority remained sufficiently restrained to avoid appearing politically sovereign. Those assumptions no longer hold securely.
What followed after the pandemic proved equally corrosive, though in a different register. The later years of the Biden administration increasingly projected not institutional confidence, but managerial exhaustion and strategic drift. Public health governance appeared trapped between reputational defensiveness, bureaucratic inertia, and political risk aversion. Agencies that had exercised extraordinary authority during the emergency phase of the pandemic now seemed unable to recover either strategic clarity or public trust. The result was a perception — fair or unfair — of an administrative order no longer fully capable of decisive self-correction.
The current phase represents something more radical still. Under the banner of institutional accountability and democratic restoration, large sections of the administrative structure are now being subjected not merely to reform, but to deliberate destabilization. Leadership continuity has weakened. Scientific authority has fragmented. Experienced personnel have departed. Interim governance has become normalized. The governing assumption increasingly appears to be that existing institutions are beyond meaningful reform and that legitimacy can therefore be restored only through disruption severe enough to break the existing bureaucratic culture.
By the time the COVID-19 pandemic arrived, confidence in Congress, universities, media organizations, and financial institutions had already deteriorated significantly across American civic life. The pandemic transformed that latent distrust into direct contestation over expert authority itself.
Yet states rarely emerge strengthened from prolonged assaults on institutional continuity. The danger in such moments is that societies convince themselves they are clearing away corruption when, in reality, they may be exhausting the very administrative capacities upon which modern governance depends. Institutions can survive criticism. They can survive reform. What they struggle to survive is the simultaneous collapse of public trust, internal confidence, leadership continuity, and procedural stability.
What now appears underway is not conventional institutional reform, but a crisis of regime confidence within the administrative state itself. During the pandemic, public health institutions expanded their authority dramatically and often exercised it clumsily. In the years that followed, the governing establishment appeared unable either to defend its decisions persuasively or to restore public trust through visible accountability. The result was a vacuum of legitimacy into which a more openly destructive political impulse has now entered.
The danger is that parts of the American political system no longer seem interested merely in correcting institutional excesses, but in discrediting the institutional structure as such. This is a historically perilous transition. States can survive bureaucratic failure. They can survive scandal, reform, even corruption. What they struggle to survive is the normalization of elite disbelief in the legitimacy of their own governing machinery. Once political actors begin treating core institutions primarily as hostile territory to be conquered, purged, or hollowed out, administrative continuity itself begins to erode.
Public health governance depends upon forms of social trust that cannot easily be reconstructed once exhausted. Scientific agencies require continuity of expertise, procedural legitimacy, stable chains of authority, and a public still willing to distinguish between institutional failure and institutional invalidity. A society may reform distrusted institutions. It may constrain them, restructure them, or subject them to greater democratic oversight. But once a political culture loses confidence in the legitimacy of expert authority itself, governance becomes increasingly reactive, fragmented, and unstable. Under such conditions, even technically competent institutions struggle to coordinate public behavior during crisis because their authority is no longer experienced as legitimate, but as merely factional or coercive.
This explains why leadership instability at HHS matters beyond ordinary political turnover. Interim leadership arrangements may suffice within agencies whose authority derives primarily from statutory enforcement. But healthcare institutions operate differently. Their effectiveness depends upon continuity, credibility, and public confidence accumulated gradually over time. When scientific agencies appear internally politicized, administratively unstable, or strategically incoherent, their guidance loses persuasive authority precisely when social coordination becomes most necessary.
Historically, advanced societies rarely lose institutional capacity all at once. More commonly, they experience a subtler form of deterioration: the erosion of confidence in the legitimacy of governing structures themselves. The late Roman Empire retained administrators long after political cohesion weakened. The Soviet Union possessed immense technical expertise even as public faith in institutional authority collapsed. Decline often begins not with the disappearance of competence, but with the weakening of the social conditions under which competence can command obedience.
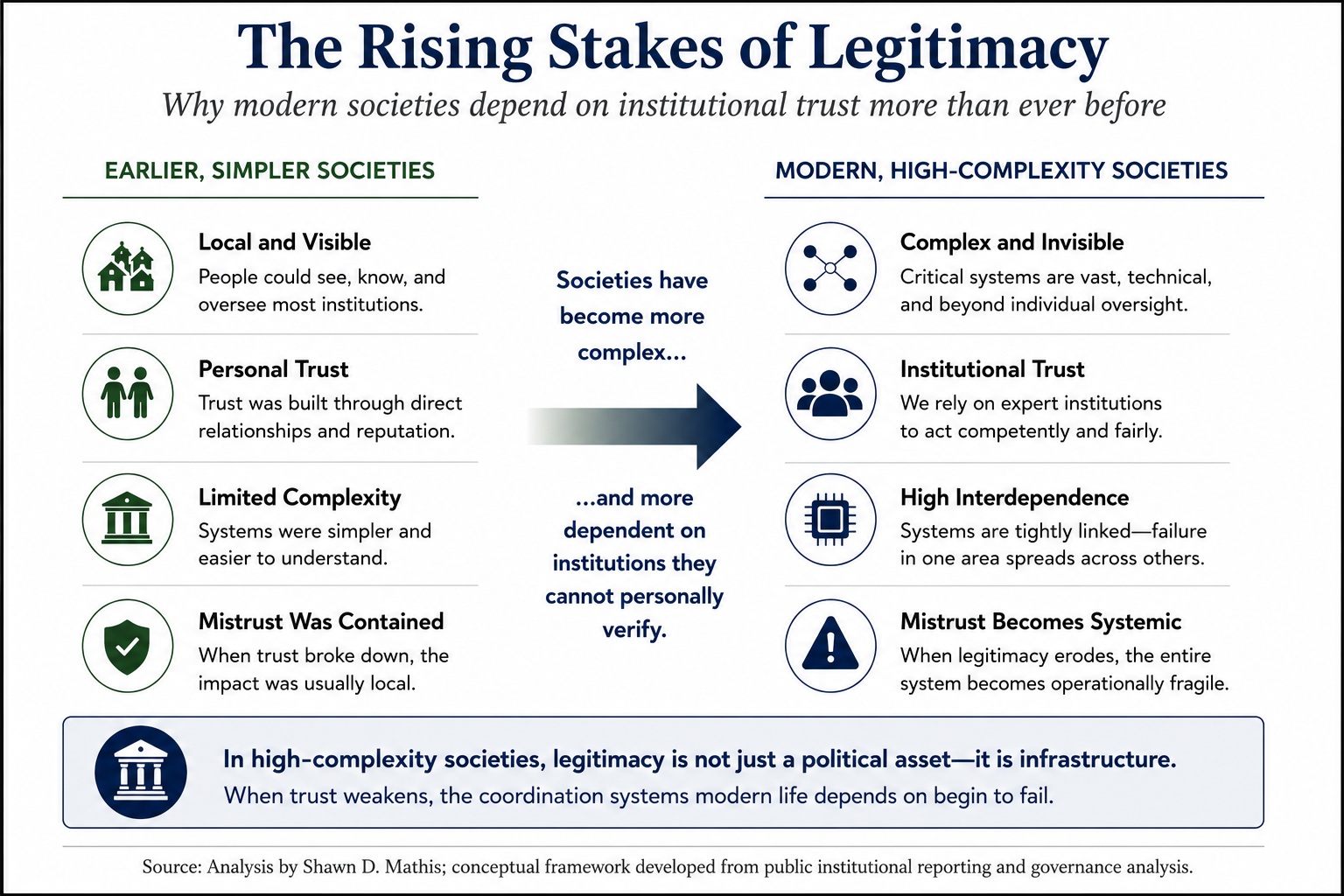
Advanced societies become more administratively capable even as they become more legitimacy-dependent. Earlier political systems could survive substantial distrust because large portions of social life remained locally governed, decentralized, and comparatively simple. High-complexity societies operate differently. Modern citizens depend daily upon technical systems they cannot independently verify and institutions they cannot personally oversee. Under such conditions, legitimacy itself becomes a form of critical infrastructure. Once trust deteriorates sufficiently, the coordination mechanisms upon which advanced societies depend begin to weaken simultaneously.
The stakes of legitimacy rise as societies become more technologically and administratively complex. In low-complexity societies, institutional distrust could often be absorbed locally without threatening the broader functioning of the state. In high-complexity societies, however, declining trust increasingly disrupts the coordination mechanisms upon which modern governance itself depends.
The United States is not facing systemic collapse. But it is confronting a genuine legitimacy problem within sectors of its administrative state, particularly those dependent upon public trust and scientific authority.
This creates the defining governance dilemma of advanced democracies in the twenty-first century. Expert institutions require insulation from transient political passions in order to function competently. Yet democratic societies increasingly distrust institutions perceived as culturally detached, ideologically homogeneous, or insufficiently accountable to public sentiment. The result is a legitimacy trap from which neither technocratic insulation nor populist intervention provides a fully satisfactory escape.
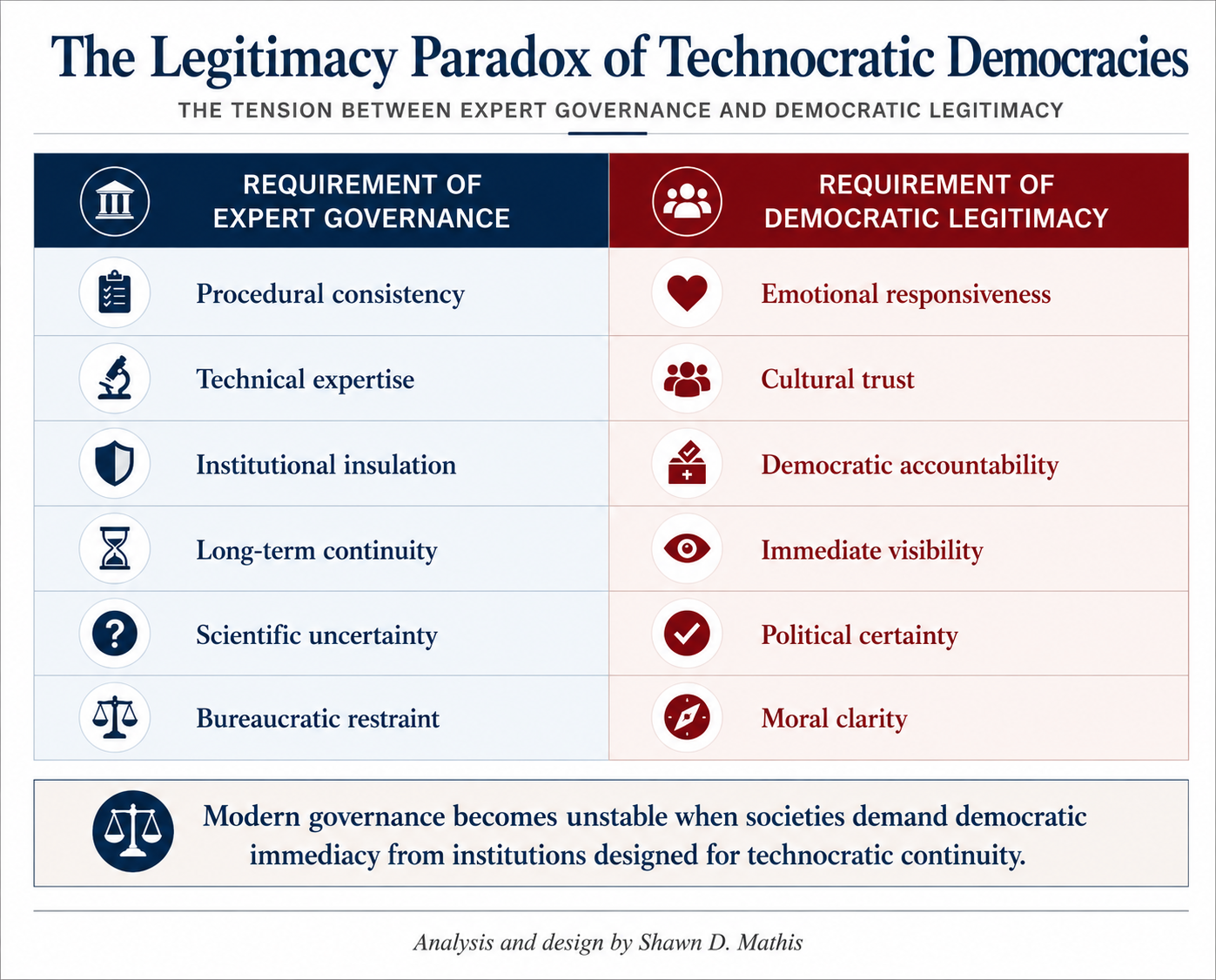
The central problem may ultimately be structural rather than merely political. Advanced democratic societies increasingly depend upon expert institutions to manage forms of complexity beyond the capacity of ordinary electoral systems to govern directly. Yet democratic legitimacy itself is becoming increasingly emotional, immediate, and culturally polarized. The result is a widening mismatch between the conditions under which technocratic institutions operate and the conditions under which democratic publics now grant trust. Modern societies require expertise more than ever while simultaneously becoming less capable of sustaining the legitimacy structures upon which expert governance ultimately depends.
If agencies become more insulated, they are accused of operating beyond democratic control. If they become more politically responsive, they appear scientifically compromised. If they communicate cautiously, they seem evasive. If they communicate aggressively, they appear ideological. Under such conditions, institutional authority erodes regardless of the path chosen.
The essential question is whether institutional legitimacy can be restored. It can, but only if expert institutions recover the discipline of procedural modesty. Public trust cannot be rebuilt through messaging campaigns, reputational management, or increasingly moralized appeals to expertise. Public trust returns when institutions demonstrate visible restraint, intellectual honesty, transparency regarding uncertainty, and a renewed commitment to remaining institutionally narrower than the ideological ambitions of the coalitions surrounding them.
At the same time, democratic societies must recover a distinction they increasingly struggle to maintain: skepticism toward institutions is healthy; total disbelief in institutional legitimacy is destabilizing. A society incapable of trusting any expert authority ultimately becomes ungovernable in moments of crisis.
The ultimate lesson of the present HHS turmoil is therefore constitutional rather than administrative. Modern healthcare systems depend not only upon medical infrastructure or scientific innovation, but upon the legitimacy of the institutions that coordinate them. Once confidence in those institutions weakens sufficiently, technical competence alone becomes insufficient to preserve authority.
The resignation of an FDA commissioner matters not because one official departed office, but because it reveals a deeper and more dangerous reality: modern democracies still depend upon expert institutions for social coordination, yet increasingly lack consensus about the conditions under which expert institutions continue to command legitimacy, public trust, and social authority.