The Collapse of Primary Health Care in the U.S.



Author's Note: During my own work in healthcare leadership and health systems, I have repeatedly encountered physicians who describe the same frustration: the growing inability to practice continuity-based care within systems increasingly organized around transactions, documentation requirements, and productivity metrics. While the particulars vary, the underlying concern is remarkably consistent. The institutional structures surrounding primary care often reward activity more readily than relationships.
The United States spends more on healthcare than any other country in the world. Yet Americans struggle to secure one of the most basic functions a healthcare system is supposed to provide: sustained access to a primary-care physician. In many metropolitan areas, patients now wait weeks or even months for routine primary-care appointments. Rural communities continue losing doctors entirely, while many clinicians are retiring early or moving into concierge models serving smaller populations outside conventional insurance systems. At the same time, rates of chronic disease, obesity, diabetes, and behavioral health dysfunction continue rising across nearly every demographic group.
These developments are often discussed as separate problems. They are not. They reflect a structural imbalance built into the American healthcare economy over decades. The system evolved to reward intervention, specialization, and procedural volume while systematically underinvesting in continuity of care.
Primary care occupies an unusual position in medicine because its value is cumulative rather than transactional. It prevents downstream crises that often never become visible precisely because they were prevented. Economically, this creates a problem. Healthcare systems organized around measurable transactions reward acute intervention more easily than long-term patient management.
This was not entirely irrational. Over the past half century, American medicine became extraordinarily effective at specialized intervention. It developed world-leading capabilities in surgery, diagnostics, oncology, pharmaceuticals, trauma care, and complex procedures. Much of this innovation produced genuine advances in human longevity and medical capability.
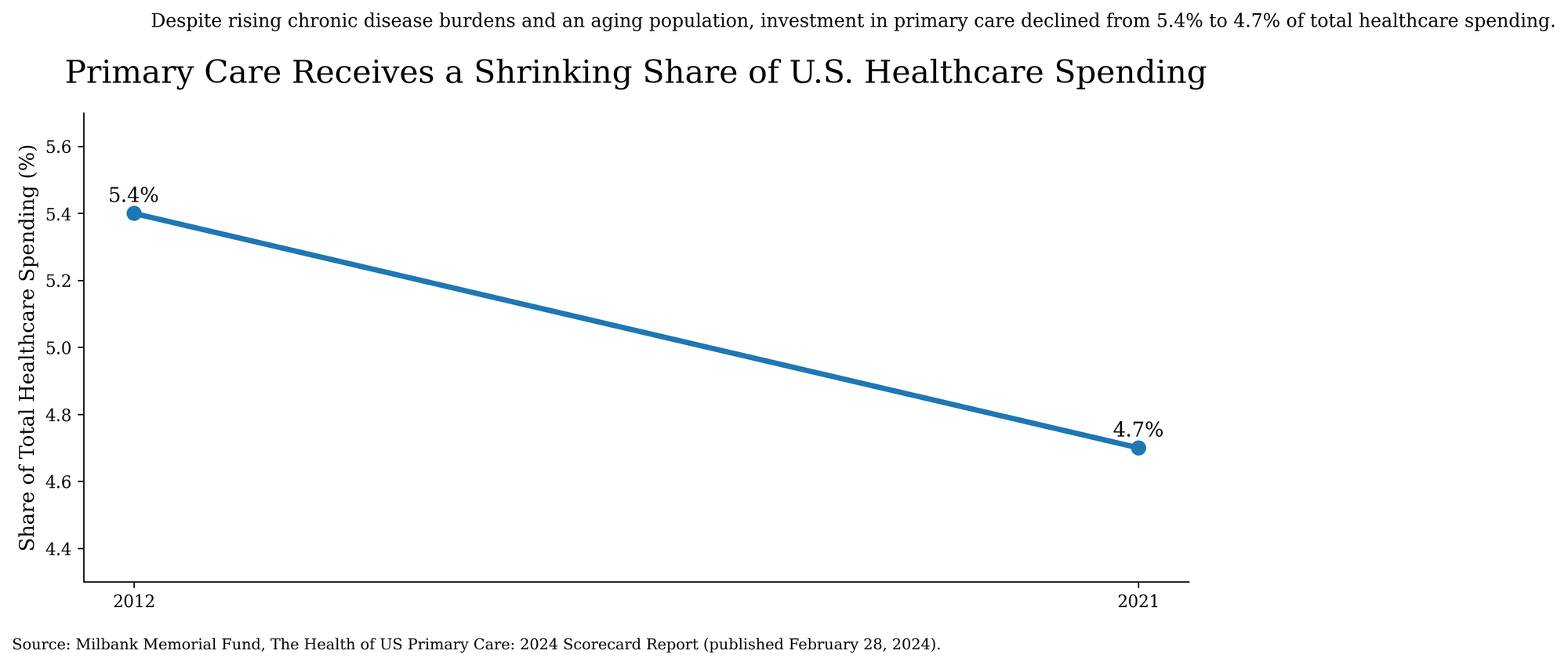
But the system also evolved around a clear financial logic: intervention is billable in ways continuity often is not. A physician performing a procedure generates measurable revenue. A primary-care doctor preventing hospitalization through long-term management generally does not. Over the past four decades, prestige, investment, and institutional influence migrated toward the sectors producing higher financial returns. Healthcare spending increasingly reflects the system’s underlying priorities. Recent analysis from the Milbank Memorial Fund illustrates the trend clearly.
The consequences are now visible. Primary care physicians are expected to manage prevention, chronic disease, medication coordination, behavioral health screening, referrals, insurance navigation, and long-term patient oversight while operating inside systems dominated by administrative burden and reimbursement compression. Many clinicians now spend substantial portions of their day interacting not with patients, but with documentation systems, coding structures, compliance requirements, and prior authorization processes.
This produces predictable outcomes. Fewer medical students choose primary care. Existing physicians leave earlier. Independent practices disappear into larger systems. Patients move between disconnected providers as long-term relationships deteriorate across insurance networks, corporate ownership structures, and increasingly specialized systems of care.
The rise of concierge medicine is particularly revealing. Public discussion often portrays concierge care primarily as a luxury preference for affluent patients. It also reflects a broader shift: an attempt by physicians to reconstruct conditions under which long-term care remains possible. In effect, affluent patients are purchasing insulation from overloaded healthcare systems.
That observation matters because it suggests the problem is not simply physician shortage. It reflects a system misaligned with the demands of primary care. Many physicians no longer believe the existing reimbursement and administrative structure supports serious primary care at scale. When institutional professionals systematically exit large systems in order to recover conditions necessary for sustained patient care and professional autonomy, the problem is usually architectural rather than individual.
Historically, this pattern is not unique to healthcare. Institutions often weaken when the activities most necessary for long-term stability produce fewer immediate measurable returns than the activities surrounding them. Financial systems become transactional. Universities prioritize expansion over intellectual formation. Public bureaucracies drift toward procedural compliance rather than mission effectiveness. Healthcare now reflects a similar imbalance.
The paradox at the center of American medicine is difficult to ignore. The United States has built one of the world’s most technologically sophisticated healthcare systems while weakening the part of the system best positioned to sustain continuity over time: primary care.

Primary care once provided stability inside the broader healthcare system. Patients did not merely receive episodic treatment. They developed ongoing relationships with physicians who accumulated contextual understanding over years, sometimes decades. That continuity improved diagnosis, treatment adherence, chronic disease management, and preventive care. It also preserved the sense that large institutions remained accountable to individual patients.
As continuity weakens, healthcare becomes more technologically capable while often feeling less coherent to the people moving through it. This helps explain why public trust in healthcare institutions has become unstable. The problem is not simply misinformation or political polarization. Many Americans no longer experience healthcare through relationships. They experience it through systems.
The distinction matters because systems built primarily around transactions eventually struggle to sustain long-term patient care. Yet aging populations and chronic disease societies depend increasingly on precisely that kind of continuity. This is why the collapse of primary care cannot be solved merely through expanded medical school enrollment or marginal reimbursement adjustments. Those measures may help, but they do not address the deeper structural issue: the American healthcare economy assigns greater institutional value to intervention than to continuity itself.
That hierarchy was sustainable when infectious disease and acute medical crises dominated healthcare demand. It is considerably less sustainable in a society shaped by chronic disease, aging populations, behavioral health pressures, and long-duration management problems. In effect, the healthcare system evolved for episodic intervention while the population evolved toward continuous management needs.
The broader conclusion is difficult to avoid. Advanced societies often become highly sophisticated at solving technical problems while weakening the institutions responsible for maintaining continuity over time. Primary care now reflects that larger pattern.
America did not accidentally neglect primary care. It built a healthcare economy in which continuity carried less institutional value than intervention. The consequences of that decision are now visible across cost, access, physician retention, chronic disease management, and public trust. Technological sophistication cannot indefinitely compensate for the erosion of continuity within systems that ultimately depend upon it.