Leading Change Under Constraint: Rethinking Leadership in the Democratic Republic of Congo



In April 2026, I led a three-part seminar series titled “Leading Change in Complex, Resource-Constrained Health Systems: The Reality of the DRC.” Hosted by the Higher Institute of Nursing Sciences (ISSI), the series brought together healthcare professionals working in conditions that resist easy description, and perhaps easy resolution. They did not, for the most part, describe these conditions directly; they worked within them.
A total of 57 healthcare professionals, primarily nurses, completed the seminar series.
The sessions began, as such things often do, with a framework; they did not remain there for long. Ideas were taken up, tested against practice, and, in some cases, quietly set aside. What remained was shaped less by presentation than by exchange—by the steady pressure of experience brought into conversation with theory.
Now, as I approached the final session, there was a sense—difficult to name, but nonetheless present—that the work had already begun to shift. Not in any decisive or measurable way, but through the gradual accumulation of understanding that occurred when reflection was held alongside practice. The framework, though still present, had receded. It remained, but no longer in the foreground. In its place was something less defined, but perhaps more durable:
a shared attentiveness to the conditions within which action becomes possible.
Co-taught with Dr. Junior Mudji—whose translation into French conveyed not only language but meaning across contexts—the sessions developed gradually, shaped as much by participant response as by design. Dr. Mudji is a physician and Director of Residency Training at Vanga Evangelical Hospital, a major referral center in Kwilu Province in the Democratic Republic of Congo, and a leading voice for quality improvement in the region. His clinical work, including his internationally recognized experience in treating conjoined twins, has been highlighted by the BBC. He holds an MSc in Global Healthcare Leadership from the University of Oxford, where he integrates evidence-based practice from the Nuffield Department of Primary Care Health Sciences with leadership theory from Saïd Business School to advance sustainable improvements in healthcare delivery. His work, like that of many in the region, moves between constraint and possibility.
Our collaboration extends beyond this seminar series. We first met in 2022 at Saïd Business School, University of Oxford, while studying for the MSc in Global Healthcare Leadership. Since then, we have worked together to deliver leadership-focused teaching to more than 120 physicians across the Democratic Republic of Congo, focusing on the practical realities of leadership in clinical settings. Over time, the distinction between teaching and learning became less clear. This ongoing collaboration informed both the content and tone of the seminar, grounding it in a shared commitment to applied leadership in context.
The teaching modules drew on work developed through the Institute for Global Healthcare Leadership (IGHL), founded by Dr. Shawn D. Mathis, and were adapted to the context of the Democratic Republic of Congo. What follows reflects the structure from which the discussions first emerged. The full presentation from the seminar series is included here for reference, reflecting the structure from which these discussions developed.
From the outset, we examined a common assumption: that change fails because people lack knowledge. In practice, this explanation proves insufficient. Across the settings discussed—hospitals operating with limited resources, persistent staffing shortages, and conditions that shift from day to day—there is no shortage of expertise. Instead, change more often falters under the combined pressures of complexity, misalignment, and constraint.
This distinction matters because it shifts the focus of leadership. The question is no longer how to introduce knowledge into the system, but how to work effectively within a reality that is already dense, uneven, and frequently unpredictable. Despite these conditions, the systems described by participants continue to function.
This is not, on reflection, a trivial observation. It suggests that the life of the system is not contained entirely within its formal design. Something persists beneath it—an accumulation of practices, adjustments, and decisions that are seldom recorded but repeatedly enacted. The question, then, is not simply how systems are meant to work, but how they continue to do so at all.
It is at this point that the concept of leadership begins to change shape. Rather than being understood as authority or formal position, leadership becomes more accurately defined as the capacity to act within existing constraints in ways that produce small, meaningful, and sustained change. This is not a theoretical claim but a description of practice. Participants repeatedly pointed to situations in which action—often taken without formal mandate—mobilized existing expertise, generated trust, and gradually established credibility.
At the same time, the persistence of difficulty cannot be explained solely at the level of individual action. Much of the challenge lies in the structure of the systems themselves, particularly in the problem of misalignment. Health systems in resource-constrained settings are rarely unified entities. Instead, they are composed of overlapping layers, including government priorities, NGO programs, donor expectations, and local operational realities. Each of these elements is internally coherent, yet they do not always align with one another. Each layer is coherent on its own terms. It is in their intersection that coherence begins to loosen.
Health systems in constrained settings are rarely single, unified entities.
Each layer may be internally coherent, yet the work of leadership is often found in the space between them: aligning direction, resources, incentives, and daily practice where perfect alignment does not yet exist.
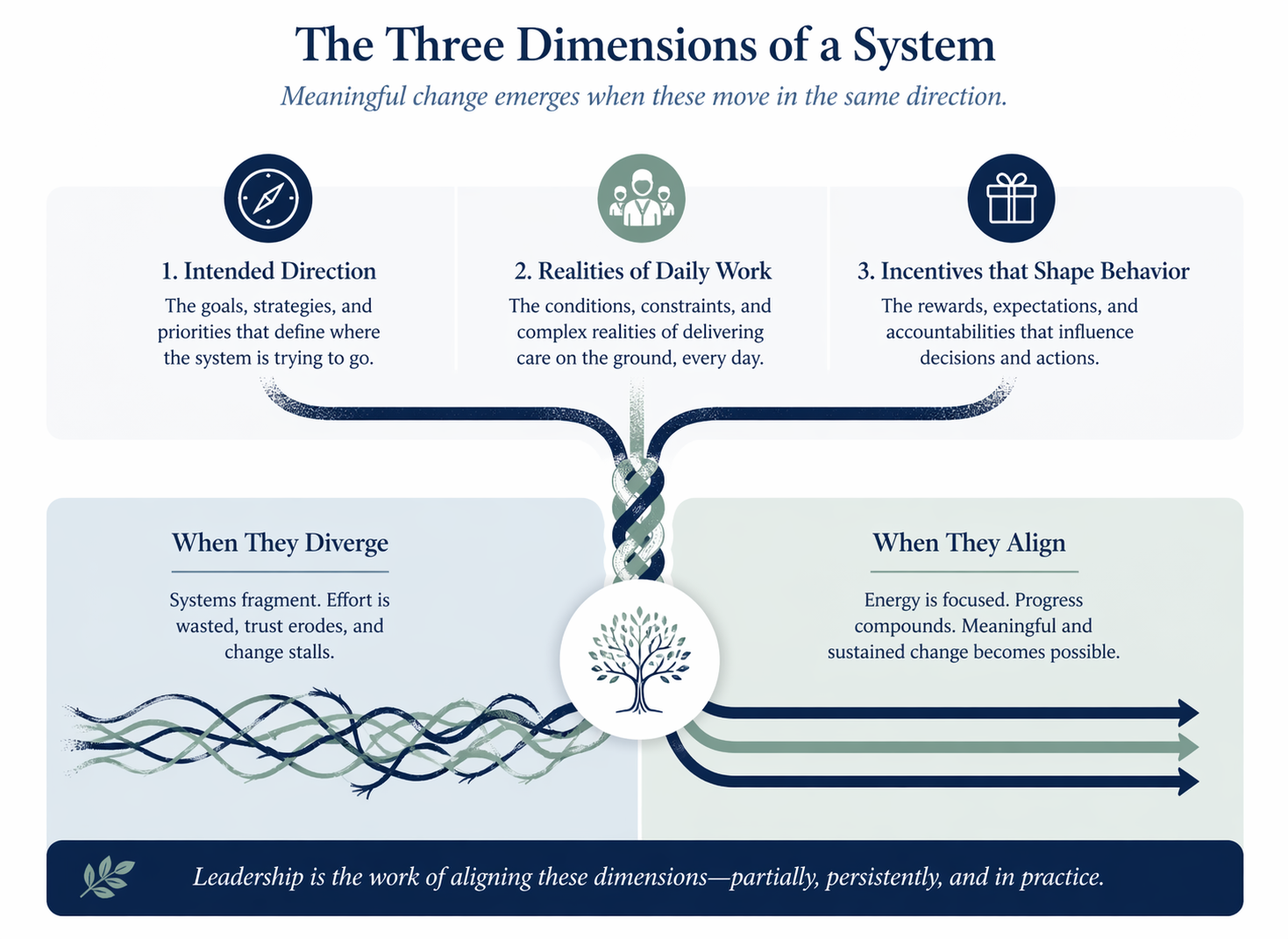
The consequences of this misalignment are visible in daily practice. Plans do not translate neatly into action, resources are not always available where they are most needed, and expectations often exceed what is feasible within existing constraints. This is not a temporary failure of coordination but a structural feature of complex systems. Leadership, therefore, cannot be reduced to setting direction alone. It requires the more practical and ongoing work of bringing elements into alignment, however partially. In the seminar, we focused on three dimensions that must be considered together: the intended direction of the system, the realities of daily work, and the incentives that shape behavior. Where these diverge, systems fragment; where they begin to align, even modestly, meaningful change becomes possible.
These ideas became more concrete through discussion of cases drawn directly from participants’ experience. One example, familiar to many, involved a patient arriving in urgent need of care when treatment was available but payment was not. The situation, as described by participants, was rarely framed as a dilemma in abstract terms. It presented itself instead as a moment—often unannounced—in which time, resources, and obligation converged without resolution.
What followed was not a single decision, but a sequence. Care might pause, not out of indifference, but out of necessity. Conversations would unfold quietly with family members, sometimes at the bedside, sometimes just beyond it. Informal arrangements would begin to take shape, shaped as much by trust as by constraint. Responsibility, in these moments, did not rest in one place; it moved—between clinician, administrator, and family—until a path forward became possible.
There is, in such situations, a kind of practiced attentiveness. Not hurried, but not slow. Not certain, but not without direction. The system, as formally constructed, does not fully account for this reality. And yet, through these small, negotiated acts, care continues.
When formal systems do not fully account for reality, leadership often appears as a sequence of negotiated actions.
A patient arrives in urgent need of care.
Care is delayed, not from indifference, but from constraint.
Clinicians and families begin the necessary negotiation.
Informal pathways form around trust, urgency, and need.
Responsibility moves across clinician, administrator, and family.
A path forward becomes possible within constraint.
What emerged from this discussion was not the uniqueness of the scenario, but its regularity. This was not an isolated case but a recurring pattern. The formal system, as designed, did not fully accommodate this reality, yet through a series of adjustments made by those within it, care was still delivered. It is precisely in these moments that leadership becomes visible—not as a formal role, but as a set of actions that allow the system to function despite its limitations.
It is at this point—where systems continue to function despite their limitations—that the question of how leaders act within constraint becomes unavoidable. This work is rarely named. It is, however, continuous.
What is required, in such moments, is not a solution in advance, but a way of seeing. The final part of the seminar turned toward the question of action within constraint. Rather than offering prescriptive solutions, I introduced the Adaptive Strategy Framework™ as a structured way of thinking through situations that participants already navigate in practice. The framework was developed during my studies in organisational leadership at Saïd Business School, University of Oxford, and emerged from an effort to translate strategic theory into a practical method for decision-making under conditions of uncertainty. It begins with the recognition of an unplanned dilemma and then requires the leader to distinguish between urgent risk and persistent risk, while also identifying what opportunity remains within the situation. In its simplest form, this is expressed as R = D × (U + P) × O, where R represents the effective reaction, D the unplanned dilemma, U the urgent risk, P the persistent risk, and O the strategic utilization of the occasion. The formulation is not intended to reduce complexity, but to discipline attention within it.
Participants’ own descriptions of their work reflected this structure with striking clarity. They spoke not in abstract terms, but in sequences: recognizing immediate threats to patient care, weighing longer-term consequences for the system, and acting with whatever resources were available while maintaining direction. The framework did not impose a new way of thinking so much as give language and discipline to what was already occurring. In this sense, it becomes less a theoretical model and more a practical method—one that enables leaders to remain composed under pressure, to act with intention rather than reaction alone, and to adjust continuously as conditions evolve. This is not an idealized model of leadership, but a grounded one, shaped by the realities of constrained systems and the necessity of acting within them. A more detailed exposition of the framework, including its theoretical development and extended formulation, is developed in my earlier work. The expression is simple; the conditions to which it is applied are not.
The action taken under pressure.
The unexpected problem requiring attention.
The immediate harm that must be addressed now.
The longer-term risk that remains beyond the crisis.
The strategic use of the occasion to move toward purpose.
One of the more important insights to emerge from the seminar concerned the scale at which change is expected to occur. There is a tendency, particularly in formal planning, to imagine change as something that arrives fully formed—visible, measurable, and decisive. In practice, it is rarely so. It proceeds instead by increments, sometimes perceptible, often not, accumulating through repeated acts that, taken individually, may appear inconsequential. Yet these small actions carry immediate effects, and over time they shape both individual capability and collective resilience. Leadership, in this sense, does not operate at the level of sweeping transformation, but through steady, ongoing adjustment.
As the seminar series came to a close, there was no single conclusion to draw. Instead, there was a shared recognition that leadership is not external to the system and does not depend solely on formal authority. It is already being practiced, often without acknowledgment, in the everyday work of navigating constraint and maintaining function within complex environments. Systems continue not because they are perfectly designed, but because people make them work.
In this light, leadership is less about control than about working alongside others to navigate constraint. It is not something distant or abstract, but something enacted in practice, repeatedly and often quietly.
The seminar given by Professor Shawn to us, various healthcare professionals spread across different provinces of the DRC thanks to the magic of technology, allowed us to understand many things about our own reality. Could this be the beginning of true leadership in our country, whose development we are still anxiously awaiting, especially in the field of health?
Although the seminar itself was bounded by three sessions, its implications extend beyond those moments. The final discussions turned toward reflection—what had worked well, what might be improved, and what could be done differently in the future. These are not questions that bring closure; rather, they point to the ongoing nature of the work.
If the series offered anything of lasting value, it was not a set of fixed answers but a way of thinking—one that remains attentive to reality, responsive to constraint, and grounded in the understanding that leadership already exists within the system. From that starting point, the work of strengthening it can continue. From that starting point, the work of strengthening it can continue—dilemma by dilemma, risk by risk, and opportunity by opportunity.