Elimination and Memory: Measles in America, Ebola in Congo, and the Problem of Maintenance


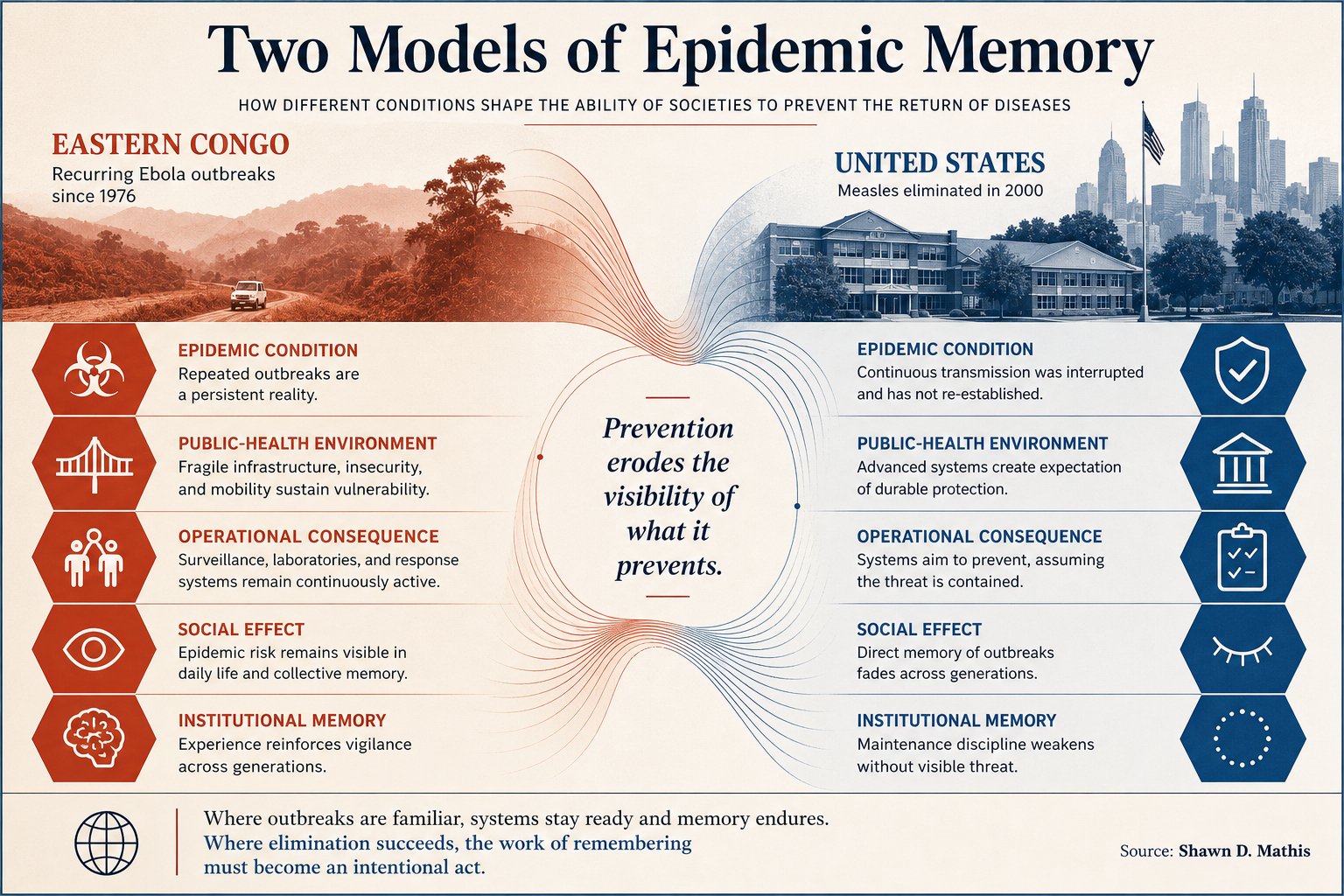
Author's Note: While researching these outbreaks, I found myself returning to a distinction that seemed increasingly important. Congo continues to manage epidemic disease as part of lived experience. In the United States, measles survives largely as historical memory. The epidemiological differences are obvious. Less obvious is the question that follows from them: whether successful prevention eventually weakens the very memory required to sustain it.
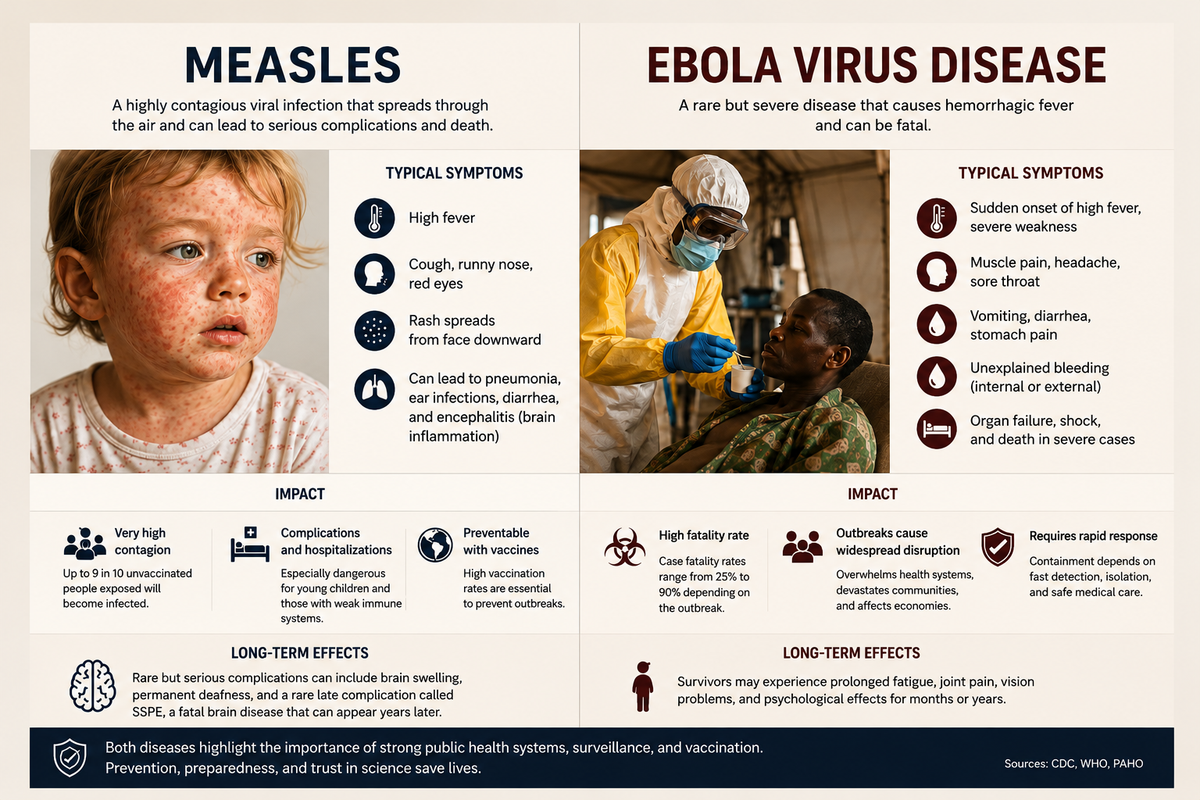
In 2000, the United States declared measles eliminated. The declaration did not mean the virus had disappeared. It meant the country still possessed the immunological and administrative capacity to prevent continuous transmission for at least twelve months, under the CDC definition of elimination. Vaccination coverage remained high enough to interrupt spread. Surveillance networks identified outbreaks quickly. Laboratories distinguished imported strains from domestic circulation. Public health authorities retained the institutional ability to contain cases before endemic transmission resumed.
That distinction matters again. By April 2026, the United States had already recorded nearly 1,800 confirmed measles cases, according to CDC outbreak reporting. International health authorities are now reassessing whether the country still satisfies the conditions required to retain elimination status under Pan American Health Organization criteria for measles elimination.
Eastern Congo faces another Ebola outbreak, as tracked by the World Health Organization and documented in PBS FRONTLINE’s Ebola in Congo. Hundreds of suspected cases have emerged in Ituri province, and Uganda has already confirmed a cross-border fatality linked to the outbreak. Health officials initially reported at least 65 Ebola-related deaths in Ituri province, according to recent reporting from The Guardian. Health officials cite mining-related mobility, insecure transport routes, incomplete contact tracing, and instability near the Ugandan and South Sudanese borders. The World Health Organization continues to classify Ebola as a recurrent regional threat requiring sustained cross-border surveillance and emergency coordination under its broader Ebola health guidance.
Elimination is not permanent. It is maintained.
Congo has never entered a post-Ebola condition. Since 1976, the country has experienced repeated outbreaks. Ebola exists there less as an unimaginable interruption than as a recurring threat managed under persistent fragility. Laboratories, border teams, treatment centers, and international agencies operate with the assumption that another outbreak will eventually occur.
The United States developed the opposite assumption. Measles elimination encouraged the belief that the disease belonged to history. Generations emerged without direct memory of crowded pediatric wards, school closures, or widespread outbreaks. The triumph over measles produced one of the conditions for its return: the disappearance of the memory that had sustained routine vaccination.
Success weakens the memory that made maintenance politically possible.
Health systems function most effectively when the dangers they suppress remain culturally visible. Once those dangers disappear from ordinary experience, maintenance begins to look optional. Vaccination shifts from civic expectation toward individualized preference. Official guidance now competes with fragmented information systems organized less around verification than around immediacy, affinity, and suspicion toward centralized authority.
Herd immunity against measles generally requires vaccination rates above 90 to 95 percent because the virus is extraordinarily transmissible. Even localized reductions can sustain outbreaks. Measles outbreaks often persist not because vaccination collapses nationally, but because exemptions and under-immunization cluster locally enough to sustain transmission chains. Researchers describe measles as a “canary in the coal mine” for broader immunization weakness, according to recent CDC measles outbreak data. A resilient vaccination regime absorbs imported cases without prolonged spread. A weakened one cannot.

The epidemiology is relatively clear. The politics are not.
Elimination status is often treated as a symbolic achievement conferred once and then permanently retained. In practice, it reflects continuous operational performance. Surveillance systems must identify cases rapidly. Laboratories must sequence viral lineages accurately. Immunization infrastructure must sustain high coverage over decades rather than months. Prevention works best when societies still remember what prevention prevented.
That reality helps explain the present American debate surrounding vaccines and public authority. Critics of Robert F. Kennedy Jr. argue that changes in vaccine rhetoric and federal messaging accelerated declining confidence during renewed measles transmission. Supporters reply that distrust toward health authorities long predates the current administration and reflects failures accumulated across decades rather than months.
Both explanations are incomplete.
Vaccination rates had already been declining before Kennedy assumed office. The underlying erosion therefore cannot plausibly be attributed to one official alone. Yet public rhetoric shapes behavior at the margins, and in highly contagious diseases those margins matter. Messaging carries particular importance when immunization levels already sit near thresholds critical for herd immunity.
The larger issue concerns credibility rather than personality.
For much of the twentieth century, disease-control agencies operated within cultures that granted broad presumptive authority to scientific and administrative expertise. That authority was never absolute nor free from error, political influence, or bureaucratic failure. Yet large parts of the population accepted the premise that certain institutions possessed demonstrated competence in matters requiring technical judgment and coordinated response.
Over time, however, that presumption weakened under the pressure of contradictory messaging, widening polarization, declining trust in elite institutions, fragmented media systems, and post-pandemic exhaustion — trends reflected in recent Pew Research findings on trust in government and institutions. Citizens now disagree not only about policy but about which institutions possess the authority to interpret reality credibly.
Health governance now operates inside that fractured environment. Scientific agencies retain immense technical capability while confronting widening suspicion regarding motives, transparency, and competence. Hospitals still function. Laboratories still sequence viral genomes. Universities still produce research. The difficulty lies elsewhere. A society may retain scientific expertise while losing the capacity for coordinated action.
Pathogens exploit social fragmentation with complete political neutrality.
The comparison with Congo clarifies the distinction. Congo struggles against scarcity: armed conflict, difficult terrain, weak transportation systems, and fragile healthcare infrastructure. Yet repeated Ebola outbreaks have also produced practical familiarity. Health officials possess operational experience with containment, isolation protocols, border surveillance, ring vaccination strategies, and emergency response because epidemic danger remains part of lived memory.
Congo remembers epidemic risk because it has never possessed the luxury of forgetting it.
That observation should not be romanticized. Chronic emergency extracts immense human cost. Repeated outbreaks exhaust healthcare workers, disrupt local economies, deepen instability, and strain already fragile systems. Nor does operational familiarity eliminate distrust. Ebola responses in Congo have repeatedly encountered suspicion toward national authorities and international organizations alike.
Still, recurrent exposure produces a form of realism often absent in affluent societies insulated from large-scale epidemic experience for generations.
The United States retains extraordinary biomedical capability. The difficulty lies less in scientific capacity than in sustaining the civic coordination required for preventive systems whose success depends upon continuity across generations.
Modern democracies increasingly struggle to maintain systems requiring deferred trust across generations. Citizens inherit complex administrative structures while simultaneously doubting the legitimacy of the authorities operating them. Expertise remains technically sophisticated even as confidence in expert institutions weakens.
Preventive systems fail first because they depend upon trust before crisis, a dynamic explored in debates over global health governance and institutional coordination during epidemics.
Roman roads did not disappear when Rome lost engineering knowledge. They deteriorated when the imperial system could no longer sustain routine maintenance across distance and time. Advanced systems often survive long enough to create the illusion that they sustain themselves automatically, and vaccination campaigns operate within the same historical logic.
Previous generations accepted obligations whose benefits appeared mainly through absence: absent epidemics, absent hospitalizations, absent childhood deaths. Once those memories fade, the rationale for collective maintenance becomes harder to sustain politically, particularly within cultures accustomed to interpreting risk through immediate personal experience rather than historical inheritance.
This is the paradox of successful prevention. The more effectively a danger disappears, the more difficult it becomes to explain why the systems suppressing that danger remain necessary.
Measles reveals that paradox because the virus responds rapidly to small declines in vaccination coverage. Other forms of civic erosion can remain hidden for years before consequences become measurable. Measles exposes weakening coordination quickly. Viruses do not respond to assumptions of historical progress.
The issue confronting the United States is therefore not merely the return of a highly contagious virus. It is the possibility that a society which once interrupted endemic transmission may no longer possess the civic coordination required to sustain that achievement indefinitely.
Elimination depended upon vaccination coverage, surveillance capacity, rapid response, administrative competence, and public cooperation across generations. Once those weaken, elimination itself becomes provisional.
Congo’s recurring Ebola outbreaks remind the world that epidemic disease remains a permanent feature of human history. The American measles resurgence suggests something equally important: advanced societies retain their achievements only so long as they preserve the disciplines required to maintain them.
Pathogens persist. The question is whether institutional memory persists with them.